Creatine deficiency disorders are inherited conditions that impair the synthesis or transport of creatine, leading to cerebral creatine deficiency. Creatine plays a crucial role in the brain as an energy buffer, helping maintain cellular energy homeostasis and supporting neurotransmission. There are two creatine synthesis defects—AGAT deficiency and GAMT deficiency—and one creatine transporter defect—CRTR deficiency. Intracerebral creatine deficiency typically presents with global developmental delay, intellectual disability, and behavioural disorders.
Table of contents
Cause
Creatine metabolism disorders result from mutations affecting the following genes:
- GATM (arginine:glycine amidinotransferase) in AGAT deficiency, an autosomal recessive disorder;
- GAMT (guanidinoacetate methyltransferase) in GAMT deficiency, an autosomal recessive disorder;
- SLC6A8 (creatine transporter) in CRTR deficiency, an X-linked disorder.
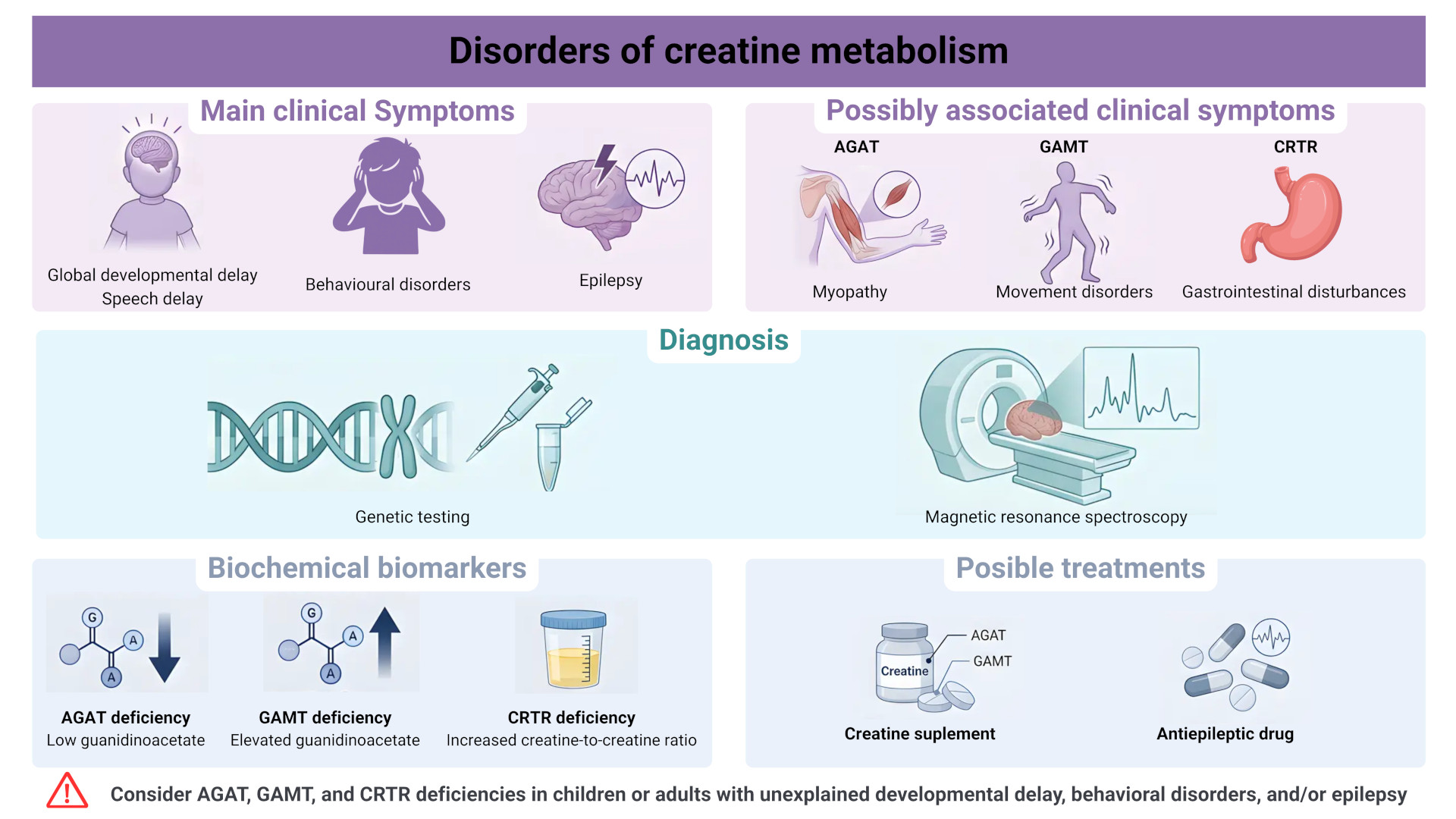
Diagnosis of cerebral creatine deficiency disorders relies on:
- brain MRI with magnetic resonance spectroscopy to assess cerebral creatine levels;
- biochemical testing: GAMT deficiency is associated with elevated guanidinoacetate, AGAT deficiency with decreased guanidinoacetate, and CRTR deficiency with an increased urinary creatine/creatinine ratio, particularly in males; and
- sequencing of the corresponding genes.
Symptoms
Clinical features include global developmental delay with speech impairment, varying degrees of intellectual disability, and behavioural disturbances such as hyperactivity or autism spectrum features.
AGAT deficiency is often associated with myopathy, whereas GAMT deficiency may be associated with epilepsy as well as hyperkinetic or dystonic movement disorders. CRTR deficiency may also be associated with epilepsy, more commonly of focal type. Although X-linked, CRTR deficiency can also affect females, with variable findings on MR spectroscopy, which may complicate diagnosis.
Treatment
AGAT deficiency responds well to oral creatine monohydrate supplementation, restoring cerebral creatine levels and improving myopathy.
GAMT deficiency requires creatine supplementation, ornithine supplementation (to reduce guanidinoacetate levels), and sometimes a low-protein diet to reduce arginine intake. The earlier treatment is initiated in childhood for AGAT and GAMT deficiencies, the better the cognitive outcome.
Currently, there is no therapy with proven efficacy for CRTR deficiency.